- Original Article
- Published:
Can open tubal microsurgery still be helpful in tubal infertility treatment?
Gynecological Surgery volume 7, pages 385–400 (2010)
Abstract
In 30 years, 1,669 patients underwent open microsurgery for tubal diseases. Several techniques like adhesiolysis, reanastomosis, fimbrioplasty, salpingoneostomy, proximal reconstruction, isthmo-ostial anastomosis and reimplantation are described. Results were excellent for patients with a favourable prognosis (1,517 patients) and with very high pregnancy rate: 80% pregnancies with delivery for tubal reversal, 68% for proximal diseases, 75.1% for fimbrioplasty and 55% for salpingoneostomy. Risks of ectopic pregnancy were very low: 1.5% for tubal reversal (because the tubes were healthy), 4% for proximal diseases, 4% for fimbrioplasty and 6.7% for salpingoneostomy. Results were very low for patients with a poor prognosis (152 patients): 10% pregnancies with delivery for distal diseases, less than 20% for proximal diseases and 22% ectopic pregnancies. Open microsurgery can still be helpful in treating tubal infertility: results are better than those obtained with laparoscopic reconstructive surgery and better than those obtained with in vitro fertilization for patients with a favourable prognosis. Patients are only operated one time and can have several pregnancies. Open tubal microsurgery is a minimal invasive surgery and saves costs (it requires a small number of instruments and minimises sutures; patients can return home 4 days after surgery, at the latest). Results on fertility are very favourable.
Between 1977 and 2007, 1,669 patients underwent a minilaparotomy for tubal diseases. Minilaparotomy means a laparotomy with minimal tissue injury, applying microsurgical principles and procedures.
One of the first principles we followed was the temporary but absolute contraindication for surgery in case of active infection and active inflammation (for example endometriotic red lesions).
We also applied the following principles:
-
gentle handling of tissues
-
atraumatic manipulation of the tubal serosa and mucosae, of the ovary and of the peritoneum
-
selective bipolar coagulation: only the vessels (and not the surrounding area) must be dessicated by fine bipolar microelectrodes
-
continuous irrigation to keep the surgical area clear at all times and to avoid the tissue from drying out (and especially the tubal serosa and the ovary)
-
perfect protection of the abdominopelvic cavity against infection risk using the sterile “wound drape”
-
complete resection of pathologic tissues
-
complete restoration of the serosa: closure of all peritoneal defects to avoid formation of de novo adhesion and recurrence of previous adhesion (peritoneal defects in case of adnexal disease due to previous infection or inflammation do not scar easily and quickly because the subserosal tissue is not a normal tissue; it is usually rich in inflammatory cells). A peritoneal closure with fine material and inverted stitches scars better and faster than a large defect without peritoneal closure
-
use of very fine resorbable sutures 7/0 and 8/0
-
last, use of a well mastered surgical technique: the surgery must be successful the first time. Repeat surgery never gives favourable results
Most of these principles were described by Gomel [1] in 1977. Open microsurgery is a method that proves to be cost efficient: the same microscope has been used for 17 years. Sets of instruments were only changed every 4 to 5 years. We only need one suture of 7/0 and one of 8/0 for two tubes. The maximum length of hospital stay is 4 days (only 3 days for 40% of the patients).
Materials and methods
Patient characteristics
Between 1977 and 1987, we operated all patients with tubal disease. One hundred and fifty-two of them had a very poor prognosis:
-
bifocal tubal lesions (distal and proximal occlusion in the same tube)
-
distal tubal lesions with poor prognosis: extended dense adhesion, sclerohypertrophic tube, intra-ampullary adhesions, lack of mucosal folds [2]
-
significant and extended proximal lesions including the isthm, the intramural segment and the ostium uterinum
After 1987, when in vitro fertilization (IVF) results became acceptable, we abandoned reconstructive surgery for these lesions and decided to perform salpingectomy in order to increase IVF results. We only operated tubal lesions with a favourable prognosis.
As a consequence, 1,517 patients with a favourable prognosis underwent reconstructive microsurgery between 1977 and 2007:
-
485 tubal reversals
-
527 distal tubal lesions
-
505 proximal tubal lesions

Materials
From 1977 to 1994, we used a Zeiss OPMI 6 microscope. A Leica-Wild M-690 was introduced after 1994. Five instruments of 15 and 18 cm long were needed:
-
two Moria forceps with very fine extremity (0.5 and 0.2 mm)
-
one Martin–Landanger microscissor
-
one Jacobson–Aesculap needle holder
-
one Codman forceps for bipolar coagulation
-
For two tubes, one 7/0 and one 8/0 polydioxanone sutures are usually sufficient.
Methods
Preoperative investigations
All patients had complete investigations: hormonal analysis, male analysis, hysterosalpingography, hysteroscopy and sometimes recanalisation, diagnostic laparoscopy with blue dye test. Results were written down before surgery and then compared with operative images (all surgery were taped first with 8-, then 16-mm film camera Beaulieu, and then with 3-CCD Sony DXC 930 P video camera) and with postoperative histological examination of all resected lesions. The analysis is therefore not entirely retrospective.
Preoperation and per operation procedures
Prior to the laparotomy, a Pezzer catheter is introduced into the uterine cavity. This catheter is brought into sterile fields and allows the preoperative injection of sterile dilute methylene blue solution for verification of the tubal patency. After a short Pfannenstiel incision (6/7 cm), we protect the pelvis with a “wound-drape”. The uterus and adnexa are elevated by packing the Douglas cul-de-sac with moistened compresses. Continuous irrigation of the surgical area using a physiological salt solution mixed with noxytioline and corticoid (permanently evacuated by a Redon drain positioned in the Douglas pouch) keeps the operating area always clear. It keeps the tissues always moistened to prevent tissue drying, avoids formation of adhesion and allows for bipolar coagulation. Extreme gentleness is exercised. Tissue traumatism is prevented by the gentle handling the tubes and the ovary with fingers rather than sharp instruments. At the end of the operating time, a meticulous cleaning of the pelvic cavity is useful.
For 30 years, several peritoneal instillates were used: Ringer's lactate which is not compatible with noxytioline, 30% dextran 70, Intergel, icodextrin 4% solution, etc., but we think it is not necessary to use instillates if the microsurgical technique is perfect: minimal tissue traumatism, perfect haemostasis, no tissue necrosis, no infection risk. We do not use these instillates in case of tubal reversal because the tubes are healthy; there is no peritoneal defect and no risk of adhesion.
Postoperation procedure
All patients (except tubal reversal) were treated with antibiotics and dexamethasone during the postoperative inflammatory time (18 to 25 days).
Patients could return home 4 days after surgery (40% of them left hospital after 3 days). Ovarian induction was prescribed after the second postoperative menstruation. Hysterosalpingography was prescribed 6 months and laparoscopy 1 year after surgery if the patient failed to conceive.
Follow-up procedure
Ninety-one percent of patients were followed up for at least 2 years. Loss of follow-up patients was classified as surgical failure because infertile women always inform their surgeon when they are pregnant or when they have an ectopic pregnancy.
Results
Formation of de novo adhesion
A minimal formation of de novo adhesion occurs after open microsurgery.
One thousand one hundred and eleven patients did not have adhesion before surgery (480 reversals, 485 proximal lesions, 146 distal lesions).

One year after surgery, 327 patients were not pregnant. Laparoscopy was performed. Filmy adhesion could be found only in 10% of patients (0 reversal, 5 proximal lesion, 27 distal lesion).
Four hundred and six patients had previous adhesion (5 reversal, 20 proximal, 381 distal). Laparoscopic checks were performed on 275 of them. While they previously presented filmy adhesion (99 patients), only 25% revealed reformation of adhesion. One hundred and seventy-six patients presented previous dense adhesion (Fig. 1). Only 23% of patients had efficient results.

Dense adhesion
In summary, only 10% revealed formation of de novo velamentous adhesion in open microsurgery. We think that adhesion formation and reformation depends on two main parameters: the quality of the surgery applying strictly microsurgical principles, which are more important than peritoneal instillates, and the aspect of previous adhesion.
Fertility after surgery
Tubal reversal
-
Technique
Reanastomosis can be isthmo-isthmic, isthmo-ampullary and ampullo-ampullary. We did not find any difference in results from using these techniques, except when the remaining tube was very short (less than 3 cm).
After resection of the tubal proximal and distal occluded ends, tubal patency was verified (Fig. 2).

Isthmo-isthmic anastomosis: section and patency of the tubal ends
The primary suture of the deep peritoneal layer of the mesosalpinx which is more difficult to perform at the end of the anastomosis must be made first. This allows the holding of the tubal segments in the proximity of one another. Two lower stitches of the muscularis submucosal layer are set at 5 and 7 o’clock with 8/0 polydioxanone; they are first set then tied at the same time (Fig. 3). The suture of this muscularis lining is completed easily by two stitches at 11 and 1 o’clock (Fig. 4).

Lower stitches of the deep musculosubmucosal layer

Upper stitches of the deep musculosubmucosal layer
Tubal patency is then tested and must be perfect. The second seromuscular layer is performed by running suture of 7/0, as well as the superficial mesosalpinx layer (Fig. 5). It is important to perform this second and superficial layer because the peritoneal healing is quickly obtained (5 or 6 days) and can protect the scar of the deep layer, which occurs later.

Isthmo-isthmic anastomosis: superficial seromuscular layer
In case of discrepancy of the tubal calibre between the isthm and the ampullary segment, the narrow segment is widened into two valves (one inferior and one superior) in order to increase the anastomosis circumference. Six stitches are set then tied at 7 and 5 o’clock, 11 and 1 o’clock and also at 3 and 9 o’clock.
In case of endometriotic proximal segment (endosalpingiosis), isthmo-isthmic anastomosis produces less pregnancy with delivery and more ectopic pregnancy. The entire proximal segment (proximal isthm and intramural segment) is resected, and an anastomosis is performed between the isthm and the ostium uterinum (isthmo-ostial anastomosis).
-
Results
Four hundred and eighty-five patients were operated.
-
Four hundred and eleven had pregnancy (84.7%) and 388 with delivery (80%);
91% of them during the first year after surgery;
seven patients needed surgery for ectopic pregnancy (1.5%).
-
Forty-five percent of patients were more than 40 years old.
-
Loss of follow-up patients (1.2%) was classified as failure.
Results of laparoscopic tubal reversal can almost have the same pregnancy rate but ectopic pregnancy rate is higher because the anastomosis is still not as perfect as in open surgery (Fig. 6: the scar of the one layer laparoscopic anastomosis is not perfect).

Laparoscopic reversal—failure due to one layer suture
Distal tubal diseases
Distal tubal occlusion can be complete (hydrosalpinx with complete atrophy of the fimbria or complete adhesion between the quasi-normal fimbria and the ovary) or incomplete (phimosis or incomplete encapsulation of the fimbria or incomplete adhesion between the fimbria and the ovary).
There are several classifications of distal tubal lesions. We use a very simple one: we consider all distal lesions with poor prognosis as contraindications of reconstructive surgery, and we recommend salpingectomy in these cases (Table 1). One of the following factors is sufficient to classify lesions as poor prognosis: dense adhesion between the tube the ovary and the peritoneum (Fig. 1), lack of mucosal folds (Fig. 7), thick tubal wall with chronic inflammation (Fig. 8), intra-ampullary adhesions covering more than a third of the ampullary area.

Lack of mucosal folds

Sclerohypertrophic tube
All other distal tubal lesions have favourable prognosis. In these cases, if the fimbria can be restored, we would perform a fimbrioplasty. If the fimbria cannot be restored correctly, it is better to sacrifice the fimbria and to perform a salpingoneostomy. This classification was already described by Palmer in 1968 [3].
-
Technique and results
We first perform a very meticulous salpingolysis: adhesions between the tube, the ovary and the ovarian pouch must be divided very kindly by microsurgical scissors to avoid damaging the ovarian albuginea and the tubal serosa. Vessels located in bleeding points are selectively coagulated by bipolar microelectrodes. Pathologic adhesion tissue must be resected. All peritoneal defects are closed by inverted stitches polydioxanone (PDS) 7/0.
Fimbrioplasty applies in three cases:
-
Firstly, sometimes normal fimbria can be completely covered by a translucent envelope (Fig. 9). In French, this lesion is called sactosalpinx. Resection of this envelope frees the normal fimbria.
Fig. 9 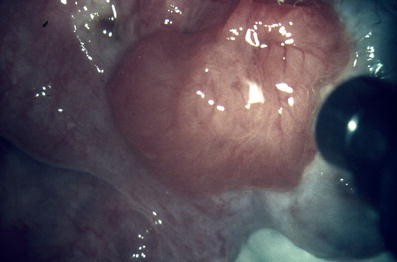
Sactosalpinx
-
Secondly, when there is an incomplete encapsulation of the fimbria. It is the first step of outside phimosis: fibrous adhesions are evolving and are progressively covering the ostium abdominale. This is called external phimosis, because it is due to fibrous adhesion. Fibrous adhesions which cover partially or quasi totally the fimbria and the infundibulo-ovarian ligament are resected. The fimbria is now free. However, the fimbria edges are folded back and secured to the serosa by inverted 8/0 PDS stitches (Fig. 10).
Fig. 10 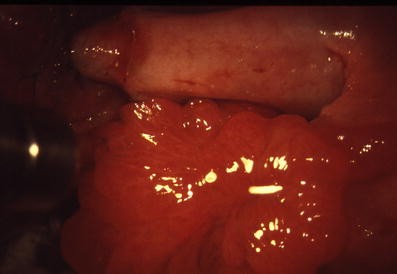
Fimbrioplasty
-
Thirdly, sometimes the fimbria is completely or incompletely occluded by an adhesion with the ovary; complete adhesion looks like a hydrosalpinx but the meticulous division between the fimbria and the ovary can free the fimbria.


However, when the fimbria is free, the ostium abdominale must be carefully inspected because sometimes, the ostium seems normal but it is very narrow or agglutinated, and it is the true phimosis (Fig. 11). Dilatation (codonolysis) is rarely successful. It is better in this case to sacrifice the fimbria and to perform a salpingoneostomy.

Phimosis
We performed 273 fimbrioplasties. Pregnancy rate was very high: 218 pregnancies (79.8%) and 205 (75.1%) pregnancies with delivery. There were only 11 ectopic pregnancies (4%). Loss of follow-up patients (4.6%) was classified as failure results.
Salpingoneostomy
We would perform salpingoneostomy when the distal extremity of the tube is totally occluded, or in case of phimosis of the ostium uterinum. The tubal occluded end is always resected, because there is always inflammatory and fibrous tissue in this tubal end.
A simple incision of avascular lines does not resect these pathologic tissues, and there is therefore a risk of recurrence. Selective bipolar coagulation of the vessels is useful. The circumference of the tubal extremity is folded back on 8 to 10 mm, and the tubal wall is everted by four to six inverted PDS 8/0 stitches (Fig. 12).

Salpingoneostomy
Results were also acceptable: 153 patients out of 254 who were operated became pregnant (60%), giving 140 deliveries (55%). Seventeen patients (out of 254) presented ectopic pregnancies (6.7%). This high rate of ectopic pregnancy can be explained by the association of distal diseases and hidden subtle lesions of the proximal segment. Loss of follow-up patients (7.8%) was classified as failure results.
Proximal tubal diseases
Proximal tubal lesions located in the isthm and the intramural segment of the oviduct were operated with macrosurgical procedures as described by Palmer [3] and Ehrler [4]. Microsurgical procedures were described by Gomel in 1977 [1], McComb and Gomel in 1980 [5], Cornier and Salat-Baroux in 1979 [6], Dubuisson and Barbot in 1983 [7], Tran in 1985, [8] in 1987 [9] and in 2007 [10], and Patton in 1987 [11].
What are proximal tubal lesions?
Proximal tubal lesions are diagnosed by hysterosalpingography and laparoscopy.
Several pictures of proximal salpingography can be described:
-
Complete proximal occlusion is called permanent (Fig. 13) when there is no tubal patency in salpingography (only a short part of the intramural segment is visible in X-ray) as well as in laparoscopy.
-
Complete proximal obstruction is called intermittent (Fig. 14) when the tube is patent in laparoscopy or in another salpingography, while there is obstruction of the ostium uterinum in the previous salpingography. The obstruction is situated in the ostium uterinum.
-
Incomplete proximal obstruction with preserved tubal patency in salpingography can be: diverticulosis (Fig. 15), rigidity of the proximal segment such as tuba erecta (tuba erecta is a classic image of vertical rigid proximal segment: Fig. 16), polyps (Fig. 17), irregularity of the tubal mucosae (Fig. 18), and mixed X-ray images (diverticulosis + irregularity + rigidity, etc.).

Complete and permanent occlusion

Complete but intermittent obstruction situated in the ostium

Diverticulosis

Rigidity of the proximal segment—tuba erecta

Polyps

Irregularity of the tubal mucosae
These images are very fine and must be examined with a magnifying glass. Between 1977 and 2002, 1,033 proximal tubes were operated. All proximal segments that were resected have had histological examination: histological section every 3 mm of the intramural segment, the isthm and the ostium uterinum (ostium uterinum is resected only in isthmo-uterine reimplantation).
Laparoscopy (Fig. 19) shows nodosa (classic salpingitis isthmica nodosa), rigidity, deformation of the cornua with intravasation in blue dye test and endometriosis of the proximal tubal serosa. Sometimes, the superficial aspect of the proximal segment seems normal.

Laparoscopic aspects
Correlation X-ray images—histology
Table 2 shows the correlation between X-ray images and histological lesions of the tube.
Amongst 1,033 tubes operated, only 3.3% of the tubes presented normal tubal wall.
The three most important illustrations of this correlation are:
-
Complete and permanent occlusion: it is an established fact that the complete and permanent occlusion always presents histological pathology of the tubal wall: fibrosis damaged 55% to 60% of tubal wall.
Recanalisation can sometimes restore the tubal patency but cannot suppress fibrosis (Fig. 20).
-
Complete and intermittent obstruction: for 67% of cases, obstruction is complete but intermittent: the lumen is temporary obstructed by mucosal agglutination, mucous debris, polyp, etc. (Fig. 21).

Complete and permanent occlusion

Complete and nonpermanent obstruction. 67% = agglutination of the lumen, mucous debris, polyp: possible to remove the obstruction by HSG, blue dye test, recanalisation; 33% operated: 8% = no lesion = spasm of Palmer
It is possible to remove the obstruction by hysterosalpingography (example of pregnancy after X-ray investigation), blue dye test and recanalisation. When these tubes (113 tubes) were operated because patient failed to conceive 1 year later, histological examination did not find any lesion in the tubal wall for 8% of the cases. Palmer called it “proximal spasm”.
-
Proximal nodosa and its X-ray diverticulosis (Fig. 22) correspond to endometriosis in only 30% of the cases, while several publications consider diverticulosis characteristic of tubal endometriosis.

Diverticulosis—fibrosis (40%), endometriosis (33%), proximal salpingiosis: outpouchings of tubal epithelium (21%), endometrial colonisation (6%)
A significant majority of the incomplete obstruction also presents histological pathology of the mucosae and the muscular layer. So, successful tubal canalisation provides correct tubal patency but cannot treat the pathologic tubal wall.
Classification of proximal diseases
Classification of proximal tubal lesion must take in account two aspects of the tube: macroscopic and microscopic histological lesions.
Macroscopic aspect is based on three factors:
-
topography of the lesion, limited or extended in length isthm ± intramural segment ± ostium and in depth: pure mucosal lesion or mucosal lesion ± muscular lesion ± serosa
-
laparoscopic aspect: nodosa, tubal deformation, tuba erecta, normal aspect
-
tubal patency (complete occlusion or incomplete obstruction)
Microscopic histological anomalies are described in Table 2:
-
fibrosis (54.5%; Fig. 23)
-
endometrial colonisation (endometrial mucosae inside the intramural ± isthmic segment but no endometriosis in the tubal wall = 3.2%; Fig. 26)
-
isolated polyp (4.3%)
-
tuberculosis (0.5%)
-
and a special lesion: proximal salpingiosis (15.5%; Fig. 27) This proximal salpingiosis reveals diverticulosa which are outpouchings of tubal epithelium (not uterine epithelium), and hypertrophic smooth muscle can surround these diverticulosa. Several synonyms have been suggested: diverticulosis (but diverticulosis is only an X-ray image and does not suggest a specific histological aspect); salpingitis isthmica nodosa (but the origin is not only infection, it can be also inflammatory; the intramural is more frequently included in the nodosa than the isthm; and this lesion does not always correspond to a nodosa); tubal adenomyosis (but diverticulosa are not glands, they are only outpouchings of the tubal lumen); endosalpingiosis (but endosalpingiosis was described by Sampson to design endometriosis of the proximal segment of sterilisation procedures).

Fibrosis

Endometriosis of the tubal wall

Endometriosis of the tubal wall

Endometrial colonisation

Proximal salpingiosis
These synonyms do not reflect the real histological aspect of this lesion.
We propose to simply call it proximal salpingiosis. We can see in Table 2 that there is no specific histological lesion for any X-ray image.
What is the choice of the treatment?
Since 1987, we have not operated highly extended lesions with great deformation of the cornua including the isthm, the intramural segment and the ostium (Fig. 28). We can make a difference in diagnosis between extended and nonextended by using X-rays and through the laparoscopic aspect (Table 3).
We have operated immediately permanent and complete proximal occlusion (tubal canalisation does not seem necessary because histological lesion of the tubal wall is always found).

Extended proximal disease
We have operated intermittent complete obstruction and incomplete obstruction with tubal patency preserved when the proximal tubal segment was pathologic: nodosa, deformation, intravasation, when these patients were infertile and there was no other factor of infertility; because tubal patency did not mean tubal normality and because these patients presented a high risk of ectopic pregnancy [12–15].
If intermittent complete obstruction and incomplete obstruction with tubal patency preserved corresponded to a normal aspect of the cornua in laparoscopy, we performed recanalisation, and used medical treatment (danazol, GnRH agonist, progesterone during 3 months followed by ovarian stimulation). If pregnancy did not occur 1 year after medical treatment (and if the patient was still young), we operated these patients.
Techniques
Three personal techniques were described in 1985 [8, 10]: Isthmo-ostial anastomosis (I.O.A), isthmo-ostial reimplantation (I.O.R) and isthmo-uterine reimplantation (I.U.R).
Isthmo-ostial anastomosis is the anastomosis between the ostium uterinum and the isthm. This is different from the isthmo-cornual anastomosis because a pathologic portion of the intramural segment could still remain in the cornua.
For the I.O.A, we first only resect the pathologic segment of the isthm and the complete intramural segment (which is always pathologic; Fig. 29). The section of the distal isthm must be performed in a healthy zone, but the prognosis is better if a long segment of the isthm can be preserved [16]. To resect completely the intramural segment, cornual resection by performing a tunnel in the cornua was described by Palmer. This tunnel can prevent uterine rupture in case of pregnancy. Haemostasis is obtained by minimal bipolar coagulation. Then, the basis of the tunnel is temporary everted by 7/0 stitches. The ostium uterinum becomes superficial and more accessible for the surgeon (Fig. 30). Patency of the ostium is verified. An initial mesosalpingeal suture approximates the isthm to the ostium uterinum. Two 8/0 polydioxanone extramucosal stitches are inserted at 5 and 7 o’clock. When these sutures are positioned, knots can be tied. Then, two similar stitches at 11 and 1 o’clock are performed (Fig. 31). Tubal patency must be perfect. The superficial seromuscular layer is now performed with 7/0 running suture (Fig. 32).

Isthmo-ostial anastomosis: dissection of the intramural segment

Isthmo-ostial anastomosis: eversion of the cornua

Isthmo-ostial anastomosis: deep musculosubmucosal layer

Isthmo-ostial anastomosis = seromuscular layer
I.O.R is performed when the ostium is not patent. The procedures are similar but only the external muscular ring of the ostium uterinum is preserved (Fig. 33). The resection of the ostium (except its external muscular ring) allows an intubation of the isthm into the ring. Patency is then better, and the physiologic role of the uterotubal junction could be preserved. The isthm must be inserted by special stitches (U knots) inside the external muscular ring until the tubal mucosae reaches the endometrium (Fig. 34), in order to avoid a postoperative fibrosed area which can be a blockage factor.

Isthmo-ostial reimplantation: resection of the ostium except its external muscular ring

Isthmo-ostial reimplantation: insertion of the isthm inside the external muscular ring of the ostium
For I.U.R, the procedures are also similar but all of the three layers of the ostium uterinum are sacrificed. It is not a good technique. The risk of recurrence of blockage is very high (more than 50%).
Results
Intrauterine pregnancy occurred for 74.8% of the patients (378/505). Sixty-eight percent of patients had live birth (343/505). There were 20 ectopic pregnancies (4%). Loss of follow-up patients (4.5%) was classified as failure results.
Conclusions
Open tubal microsurgery is really a minimal invasive surgery and can still be an excellent technique for most of tubal diseases. There is no competition between tubal microsurgery and IVF; they are complementary.
For tubal reversal, microsurgery must be performed first because pregnancy rate is very high. IVF cannot give same results, especially when 45% of patients are more than 40 years old (patients above 40 years of age had tubal reversal because they were still fertile, and their tubes were still healthy). There was no significant difference with regards to age on pregnancy results (but we did not operate patients above 43 years old). For distal and proximal diseases, patients of 40 years old are usually patients with poor prognosis and cannot be operated (distal lesions can be quite old and can create the atrophy of the mucosae; old proximal disease can be extended). In the future, laparoscopic reversal could present same results for pregnancy with delivery but ectopic pregnancy rate must be reduced by use of fine sutures (8/0), fine instruments and best technique of suturing [17].
For distal tubal lesions, more than 50% of the patients have a poor prognosis. These tubes must be resected in order to increase favourable results for IVF. On the other hand, distal lesions with favourable prognosis must be operated first. In case of failure, IVF can be performed 1 year after surgery (Table 1). Laparoscopic surgery cannot presently give same results because laparoscopic adhesiolysis is still too traumatic, and electrocoagulation damages too much tubes and ovaries. It is also important to use an optimal suturing technique.
For proximal lesions, about 30% of patients have poor prognosis. They must have IVF, but it is usually uterine adenomyosis extending to the tubes; and IVF does not yield favourable results. Proximal lesions with favourable prognosis must be treated first by microsurgery, followed by IVF 1 year later if the patient is not older than 38 years of age (Table 3). In case of proximal lesions with favourable prognosis, open microsurgery is easier and more precise than laparoscopic microsurgery, even when assisted by a robot.
Several publications recommend adhesion to microsurgical principles for gynaecological surgery even for laparoscopic surgery [18–21].
References
Gomel V (1977) Reconstructive surgery of the oviduct. J Reprod Med 18(4):181–190
Boer-Meisel MF, Te Velde ER, Habbema JP, Kardaun JW (1986) Predicting the pregnancy outcome in patients treated for hydrosalpinx, a prospective study. Fertil Steril 45:23–29
Palmer R (1968) Le traitement chirurgical des stérilités tubaires. Bull Fed Soc Gynecol Obstet 20:129–210
Ehrler P (1965) Anastomose intramurale de la trompe. Un procédé nouveau de plastie tubaire pour supprimer les implantations. Bull Fed Gynecol Obstet 17:866–869
Mccomb P, Gomel V (1980) Cornual occlusion and its microsurgical reconstruction. Clin Obstet Gynaecol 23(4):1229–1241
Cornier E, Salat-Baroux J, Rotman J (1979) Implantation tubo-utérine technique microchirurgicale. Nouv Presse Med 8:2017–2019
Dubuisson JB, Aubriot FX, Barbot J, Thalabard JC, Dendrinos S, Henrion R (1983) Traitement microchirurgical des lésions proximales de la trompe. J Gynaecol Obstet Biol Reprod 12:81–86
Tran DK (1985) La microchirurgie dans la stérilité tubaire. Rev Fr Gynecol Obstet 80(11):839–840
Tran DK, Mourey C, Olivero JF, Simon E, Grimaldi M, Abrar D (1987) Traitement microchirurgical des lésions du segment proximal de l’oviduct. J Gynecol Obstet Biol Reprod 16:627–631
Tran DK (2007) Microchirurgie par laparotomie du segment proximal de la trompe. Encycl Med Chir Elsevier—Paris—Techniques chirurgicales-Gynecology 41.524:1–10
Patton PE, Williams TJ, Coulam CB (1987) Microsurgical reconstruction of the proximal oviduct. Fertil Steril 47(1):35–39
Vasil Persaud MB (1970) Etiology of tubal ectopic pregnancy. Obstet Gynecol 36:257–263
Honore L (1978) Salpingitis isthmica nodosa in female infertility and ectopic pregnancy. Fertil Steril 29:164–168
Tran DK, Leroy JL (1992) Rôle des lésions tubaires dans la genèse des grossesses extra-utérines. Hypothèses pathogéniques 31è Réunion de la Société Française pour l’étude de la fertilité. Contracept Fertil Sex 20:40–43
Majmudar B, Henderson PH, Semple E (1983) Salpingitis isthmica nodosa, a high risk factor for ectopic pregnancy. Obstet Gynecol 62:73–78
Boeckx W, Winston R, Vasquez G, Brosens I (1979) Etude clinico-experimentale des différents segments tubaires après modification micro chirurgicale. Société Française pour l’étude de la Stérilité et de le fécondité—Colloque de Bruges 1979. Oviducte et Fertilité—Masson ed. Paris, pp. 139–151
Koh CH (1998) Laparoscopic microsurgical tubal anastomosis. In Endoscopic surgery for gynecologists, 2nd edn. Ed. Saunders Company Ltd, pp. 176–185
Holmdahl L, Risberg B, Beck DE, Burns JW, Chegini N, di Zerega GS, Ellis H (1997) Adhesions: pathogenesis and prevention—panel discussion and summary. Eur J Surg Suppl 577:56–62
Canis M, Botchorisvili R, Wattiez A, Rabischong B, Houlle C, Mage G, Pouly JL, Manhes H, Bruhat MA (2001) Prévention des adhérences péritonéales. J Gynecol Obstet Biol Reprod 30:305–324
Lower AM, Hawthorn RJS, Clark D, Boyd JH, Finlayson AR, Knight AD, Crowe AM (2004) Adhesion-related readmissions following gynaecological laparoscopy or laparotomy in Scotland: an epidemiological study of 24046 patients. Hum Reprod 19(8):1877–1885
Recommendations of the Practice Committee of the ASRM and the Society of Reproductive Surgeons (2007) Pathogenesis, consequences and control of peritoneal adhesion in gynecologic surgery. Fertil Steril 88(1):21–26
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tran, D.K. Can open tubal microsurgery still be helpful in tubal infertility treatment?. Gynecol Surg 7, 385–400 (2010). https://doi.org/10.1007/s10397-010-0556-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10397-010-0556-5