- Innovative Techniques
- Published:
Improvement of endoscopically assisted neovagina: new application instruments and traction device
Gynecological Surgery volume 1, pages 133–138 (2004)
Abstract
Introduction
Despite the advantages of the laparoscopic-assisted technique of creation of a neovagina, the method is still time-consuming and has weak points. The main complications are the slipping off of the traction device, the ripping off of the threads, the unstable direction of the tension, and further technical complications.
Technical and clinical results
Through the perfected mechanics of the traction device and the application instruments all the complications due to the old mechanical system can now be avoided. The first clinical results show that using the new modern equipment leads to a significant reduction of the operation time and of the time of tension but still having the same equally good functional and anatomical results without a higher complication rate.
Conclusion
Through the new developed traction device and the perfected application instruments an operation set exists for the optimization of the laparoscopic-assisted creation of a neovagina and therefore for the therapy of a lot of cases of vaginal aplasia.
Introduction
Both the incidence and the importance of vaginal aplasia is still underestimated and sometimes a taboo; however, for the woman concerned vaginal aplasia is not only an anatomical and functional change, but also greatly affects her femininity and how she sees herself. The good news is that operative correction has become an atraumatic intervention thanks to minimally invasive methods inclusive of all advantages of this minimal invasive method such as the minimization of the trauma of the operation, a short operation time and convalescence, and a decreasing of possible complications along with the same, good anatomically and functional results [5].
The disadvantage of the commonly used Vecchietti method [1, 2] for reconstructing a new vagina in cases of vaginal agenesis was the need for laparotomy. In 1992 in the gynecological hospital of Heidelberg a new and successful endoscopically assisted creation of a neovagina [3, 4] was developed by a variation of the Vecchietti’s method. Since this time the laparotomy is not any more necessary for this kind of operation and the laparoscopic method presently is an established method. First of all, in cases of the Mayer-Rokitansky-Küster-Hauser syndrome and in many cases of testicular feminization [6, 13].
The operative creation of a neovagina is carried out if the woman expresses a wish to be able to have intercourse. Should this be the case, it is essential for the surgeon to have a profound knowledge of the anatomical changes associated with the different types of aplasia syndrome. Mayer-Rokitansky-Küster-Hauser syndrome is accompanied in approximately 38% of cases by malformations of the kidneys and the urinary tract with unilateral kidney agenesis, unilateral dystopic kidney, kidney hypoplasia or renal duplications, and ureter fissus. In approximately 20% there are malformations of the skeletal system with formation of block vertebrae in the cervical spine and the upper thoracic spine area.
In order to achieve optimal operative results, while ensuring the shortest possible operation and convalescent phase and to minimize complications associated with the technique and operation, new application instruments, including a new mechanical traction device, have been developed or optimized for laparoscopy-assisted neovagina creation. It was necessary, because the usually used technique instruments [2, 3, 4] had some important weak points such as the complicated application of the traction device which needed a long time. Also the tightening of the threads intra- and postoperatively was complicated because of the construction of the traction device. It could slip off or the threads could rip off. Sometimes a new operation was necessary to bring new threads again up to the abdominal wall. It was also necessary to shorten the time until the traction device could be removed, which needed in this time 1 week [7] or 2 weeks [4].
To avoid all these problems we developed the following questions:
-
1.
How can a traction device be constructed without problems such as (a) slipping off of the traction device, and (b) ripping off of the threads? (see Table 1)
Table 1 Experience with neovagina -
2.
How can the direction of the tension be established during a longer time and how can we tighten equally both traction threads at the same time?
-
3.
How can we improve the mechanics to shorten the time of tension?
-
4.
How can we avoid an unintentional opening of the traction device but have also at the same time the possibility to loosen it without a jerky reduction of the tension?
-
5.
How can we improve the surface of the traction device that we do not need a cushion under it and it does not hurt the abdominal wall?
-
6.
An easy way of removing the traction device and the other components is needed and the possibility of a quickly way to autoclave everything.
-
7.
What kind of different improvements of the instruments are necessary?
-
8.
What kind of and how many different dilators are needed for the primary and secondary dilation?
Methodical changes and clinical application
Improvement in mechanics, traction device, and instruments
We could develop a complete application set by improving the traction device and the applicators and by integrating a dilator for the rectum and different dummies for the postoperative use. But the most important thing is the completely new developed traction device with new mechanics and the integration of necessary regulation systems.
Traction device
Thanks to the rounded edges and the flat, solid surface, the traction device (Fig. 1) sits well on the patient’s skin without causing any significant pressure points. The extremely tolerable, biocompatible material is a plus for the patient’s comfort.

The new constructed and designed traction device (Karl-Storz, Germany)
To attach the threads to the traction device, the threads are passed along the sides of the traction device over movable rollers (to protect the thread) [1] to the spring opposite [2]. The springs also have movable rollers [3] to protect the thread. The threads are run around these and then placed in the holding device slit. After lowering the tensioning wheel [4] until a click is heard, the tension can be built up in intervals by turning the wheel. The great advantage of this is that both threads can be tightened simultaneously, and most important, evenly. Furthermore, the tensile direction is predetermined throughout the entire procedure. Partial relaxation of tension is possible at any time via the release lever [5]. Once the desired tension has been attained the tensioning wheel should be locked into position via the safety lever [6]. This safety device prevents the patient or operator from releasing the traction device unintentionally. To increase and decrease tension the safety lever must be released.
For cleaning and sterilization purposes the traction device can easily be dismantled into five parts and prepared by undoing the screws [7]. The entire instrument set can be autoclaved.
Applicators
The following applicators are part of the neovagina set:
-
1.
Thread guide straight for the vagino-abdominal perforation after Wallwiener
-
2.
Two curved thread guides, one large and one small, both with two different bends for the abdomino-vaginal perforation after Fedele or peritonealization, respectively (Fig. 2a)
Fig. 2 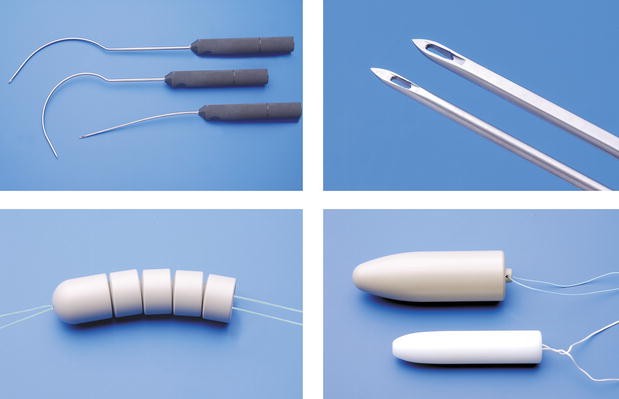
a Thread guide straight, two curved thread guides with two different bends. b The point of a needle, sharp edged with an optimized bore hole for the recommended thread: Terylene USP 4, Serag Wiessner. c Pluggable segmented dummy. d Example of a preoperative dummy and a postoperative dummy
-
3.
Pluggable segmented dummy (Fig. 2c)
-
4.
Dummies: small preoperative dummy and postoperative dummies in different sizes for individual configurations (Fig. 2d)

All the thread guides are equipped with ergonomic handles (Fig. 2a).
The curvature of the thread guide has been optimized to enable the surgeon to apply different surgical variants [3, 4, 7]. This modified curvature now also facilitates the positioning of the traction device as cranially as possible while allowing the execution of a complete peritonealization.
Positioning the device as far toward cranial as possible enables a precisely cranioventral tensile direction, thus ensuring greatest dilation potential of the neovagina as regards maximizing length (Fig. 3).

Correct marking of the exact localization of the puncture sites for the curved thread guide and also the exit points of the threads and the later correct position of the traction device
This correct position prevents an excessively ventral tension direction which tends to result in, as described in the literature [7], too short neovaginas or even bladder lesions due to luxation of the pluggable segmented dummy intraabdominally.
The distal tips of the thread guides have been improved (Fig. 2b). They are sharp-edged for ensuring a smooth perforation of the septum recto-vaginale respectively to ease the retroperitoneal positioning of the traction threads. The bore holes are perfectly adjusted to the recommended threads (Terylene USP 4, Serag Wiessner).
We had good clinical results with the intraoperatively used pluggable segmented dummy (Fig. 2c). It was adapted to the postoperatively used dummy. This pluggable segmented dummy now has only one hole which is a hygienic advantage. Like the dummies for dilation it is made of a good tolerated material and can be autoclaved.
Among the different dummies there is a preoperative dummy. The patients can use it to dilate the pseudohymen preoperatively or to practice how to use the postoperative dummy. It is important to know that in some cases not the pseudohymen is dilated but the urethra. But in these cases one cannot find a remaining incontinence, an irritation of the mucous membrane, or an increasing number of cystitis.
Finally, the set contains individually formed dummies in different sizes in order to suit the varying sizes and individual configurations of neovaginas.
At the moment there are dummies (Fig. 2d) in six different sizes available (length 10 or 12 cm; 2, 2.5, and 3 cm in diameter). They have a loop where one can fasten a thread. Because of hygienic causes the surface is completely smooth. Every set contains a little brush for cleaning the loop. So, because of the material and the surface an optimal functionality and hygiene is achieved.
The rectum dilator, also recommended for use with the set (Clermont-Ferrand model, Karl-Storz, Germany), serves to distance the rectum from the rectovaginal septum, base of the bladder, and path of the ureters, if digital distancing is insufficient.
Clinical application
Operative technique
The operative principle is based on stretching of the vaginal membrane intraabdominally. Via a pluggable segmented dummy, which is connected to two threads, pressure is continuously exerted on the vaginal membrane resulting in the formation by stretching of a neovagina within a matter of days. Using the vagino-abdominal perforation method of Wallwiener the two threads are drawn intraabdominally from the vaginal membrane using the straight single-prong thread guide, by means of which the vaginal membrane is perforated (through a single perforation), and then pulled outside the abdominal wall with a large curved thread guide which is positioned retroperitoneally from cranial to caudal. Using the abdomino-vaginale perforation method of Fedele one of the curved thread guides is used. This thread guide is also positioned retroperitoneally from cranial to caudal, then the vaginal membrane is perforated with this thread guide and the threads executing traction are threaded extraabdominal/extravaginal and then also pulled outside the abdominal wall. Outside the abdomen the threads are held taut by a traction device and tightened daily so that a constant stretching pressure is exerted on the vaginal membrane.
The vesicorectal tunnel does not have to be dissected.
Alongside optimal imaging, intralaparoscopic simultaneous cystoscopy for the purpose of diaphanoscopic–laparoscopic visualization of the exact localization of the bladder site before the vaginal perforation of the rectovaginal septum is just as essential as ruling out, by means of cystoscopy, a bladder and ureter lesion, or the intraoperative introduction of suprapubic urinary drainage. For this, the ideal positioning of the operation team is important (Fig. 4a).

a Positioning of the surgical team: typical formation of the surgical team for operative laparoscopy. At the same time, a second team inserts the threads and the pluggable segmented dummy from vaginal under simultaneous laparoscopic and cystoscopic control. b The curved thread guide is inserted retroperitoneally to pull the threads outside or to perforate the vaginal membrane using the abdomino-vaginal perforation method. c Placement of the traction device and tightening of the threads, which are connected to the pluggable segmented dummy. d Final surgical site with tensioned threads; puncture sites; suprapubic catheter and transurethral catheter and intravaginal pluggable segmented dummy located in situ
Suprapubic urinary drainage guarantees undisturbed miction despite intensive tensioning of the threads and makes postoperative introduction of a transurethral catheter during the tensioning phase unnecessary, as this could cause necrosis due to the urethra wall becoming trapped between transurethral catheter and pluggable segmented dummy.
Postoperative application
The postoperative dummy is inserted into the vagina immediately after removing the traction device and pluggable segmented dummy (Fig. 5c,d).

a Situs after removing of the traction device after a successful time of tension. b Neovagina after removing of the traction device (urethral catheter to show the urethra). c Inserting of the postoperatively used dummy after douching of the vagina. d Intravaginal dummy with very good postoperative results in length, diameter, and dilation
It must be worn for several months post-surgery in conjunction with plenty of estrogen-containing cream, full-time in the first 3–4 weeks after the operation, then at least at night. Should regular intercourse not be possible after the healing/epithelialization phase, it must be worn at least at night for several additional months, since without intercourse there remains at least the theoretical risk of secondary shrinkage of the neovagina [14].
Experience has shown that initial coitus can take place with the understanding compliance of the partner as soon as 3 weeks after the operation. The dummies can be cleaned with conventional soap or disinfecting solution.
Clinical results
Through the perfected mechanics of the traction device the operative principle of formatting a neovagina by performing a continuous pressure on the vaginal membrane with a penis-formed dummy could be maintained. Because of all these improvements, it was possible to shorten the time of tension (3–4 days), still having the same functional and anatomical results (two fingers in diameter and a length about 10 cm; Table 1).
The new mechanics of the traction device, including the new feather and thread mechanism, led to a significant reduction of the time of tension. Also many complications that were caused by the old mechanics could be avoided. There was no case with a wrong placement and a wrong direction of the tension and at least no damage or tearing off of the threads.
The special surface of the traction device does not need a cushion and does not hurt the abdominal wall.
Conclusion
The optimization of the endoscopically assisted creation of a neovagina with new application instruments and a new mechanical traction device made it possible to avoid technical problems and the following complications. There were also optimal operation results with a shorter operation time and time of tension.
To get all these optimal results it is necessary to use the newest and most modern application instruments. The easy managing of the instruments and the shorter time of tension with better results at the same time show the importance of the new instruments.
At the moment there is a prospective study at the gynecological hospital of Tübingen. It investigates to what extent the renunciation of the surgical dissection of bladder and rectum led to another optimization. This was done by an opening of the recto-vaginal septum from the abdominal side.
Regardless of the particulars of each case, however, this technique is a complex surgical-endoscopic procedure and the surgical team must have the corresponding skills.
It must be remembered that failure of the first surgical intervention diminishes the chances of the desired result . This must also be considered in the light of the great importance the neovagina and its proper functioning undoubtedly bears for the woman.
References
Vecchietti G (1965) Creation of an artificial vagina in Rokitansky-Kuster-Hauser syndrome. Attual Obstet Ginecol 11:131–147
Vecchietti G (1980) Die Neovagina beim Rokitansky-Küster-Hauser-Syndrom. Gynäkologe 13:112–115
Gauwerky JFH, Wallwiener D, Bastert G (1992) An endoscopically assisted technique for construction of a neovagina. Arch Gynecol Obstet 252:59–63
Gauwerky JFH, Wallwiener D, Bastert G (1993) Die endoskopisch assistierte Anlage einer Neovagina—Operative Technik und Erfahrungen. Geburtsh. u. Frauenheilkunde 53:261–264
Borruto F, Chasen ST, Chervenak FA, Fedele L (1999) The Vecchietti procedure for surgical treatment of vaginal agenesis: comparison of laparoscopy and laparotomy. Int J Gynaecol Obstet 64:153–158
Fedele L, Bussacca M, Candiani M, Vignali M (1994) Laparoscopic creation of a neovagina in Mayer-Rokitansky-Kuster-Hauser syndrome by modification of Vecchietti’s operation. Am J Obstet Gynecol 171:268–269
Fedele L, Bianchi S, Tozzi L, Borruto F, Vignali M (1996) A new laparoscopic procedure for creation of a neovagina in Mayer-Rokitansky-Kuster-Hauser syndrome. Fertil Steril 66:854–857
Fedele L, Bianchi S, Zanconato G, Raffaelli R (2000) Laparoscopic creation of a neovagina in patients with Rokitansky syndrome: analysis of 52 cases. Fertil Steril 74:384–389
Ikuta K, Ilda T, Okada H, Murakami, Hanada S, Yagami Y (1996) Laparoscopic-assisted creation of neovagina. J Am Assoc Gynecol Laparosc 4:53–56
Keckstein J, Buck G, Sasse V, Tuttlies F, Ulrich U (1995) Laparoscopic creation of a neovagina: modified Vecchietti method. Endosc Surg Allied Technol 3:93–95
Marwah V, Bhandari SK (2001) Laparoscopic creation of a neovagina in Mayer-Rokitansky-Kuster-Hauser syndrome by modification of Vecchietti’s procedure. J Am Assoc Gynecol Laparosc 8:416–424
Cooper MJ, Fleming S, Murray J (1996) Laparoscopic assisted Vecchietti procedure for the creation of a neovagina. J Obstet Gynaecol Res 22:385–388
Bloechle M, Sydow P, Blohmer JU, Schreiner T, Lisse K (1996) Vaginal reconstruction in vaginal aplasia by a Vecchietti modified laparoscopic operation: futher simplification of the method. Zentralbl Gynakol 118:303–306
Christensen B (2002) Minimalinvasive Möglichkeiten zur Bildung einer Neovagina. Zentralbl Gynakol:313–316
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brucker, S., Aydeniz, B., Gegusch, M. et al. Improvement of endoscopically assisted neovagina: new application instruments and traction device. Gynecol Surg 1, 133–138 (2004). https://doi.org/10.1007/s10397-004-0017-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10397-004-0017-0